Experiment # 2
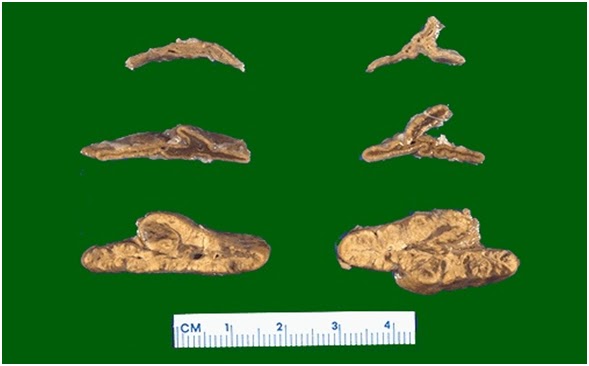
To examine a slide with an arterial atherosclerosis and thrombosis
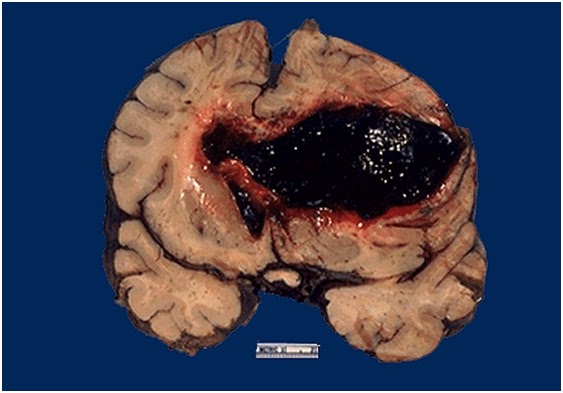
An atherosclerotic plaque can weaken the wall of an artery, potentially causing a rupture of the vessel; it can cause thrombosis (as it did here) and thereby complete occlusion of the lumen; and it can continue to "grow."
THEORY:
Atherosclerosis often develops at branch points or curving portions along extracranial and intracranial large arteries, locations where blood flow is slowed and more turbulent. The internal carotid artery is particularly at risk. Exactly where disease tends to occur, though, and how quickly it progresses apparently reflect the individual's genetic background. Additional factors that may stimulate plaque growth include hypertension and cigarette smoking.
Atherosclerosis involves focal accumulation of lipid, smooth muscle cells, foamy macrophages, and, eventually, cholesterol crystals under the surface lining (endothelium) of the artery. With time, such an accumulation can form an elevated plaque that protrudes into the vessel's lumen and significantly reduces blood flow. Perhaps the analogy of a kitchen drain pipe becoming gradually plugged with cooking grease and sludge will help to visualize what is happening.
If occluding the vascular lumen weren't bad enough, plaques can do a number of additional things that further compromise the brain's circulation. For instance, a plaque can ulcerate (break open), and the damage to its endothelial lining stimulates the development of a thrombus (blood clot) which even further narrows the vessel. What's more, pieces of thrombus or fragments of an exposed plaque core can be swept along by the blood flowing through the vessel, becoming emboli.
Atherosclerotic plaques can form in the walls of small arteries as well. However, there are several additional kinds of pathology that particularly affect the walls of small arteries leading to their collapse and blockage of blood flow.
Experiment # 3
To examine a slide of lung with a pulmonary embolus
THEORY:
Nearly all PEs arise from thrombi in the lower extremity or pelvic veins (deep venous thrombosis [DVT]. Once DVT develops, clots may dislodge and travel through the venous system and right side of the heart to lodge in the pulmonary arteries, where they partially or completely occlude one or more vessels. The consequences depend on the size and number of emboli, the pulmonary reaction, the underlying condition of the lungs, and the ability of the body's intrinsic thrombolytic system to dissolve the clots.
Endogenous lysis reduces most emboli, even those of moderate size, without treatment, and physiologic alterations decrease over hours or days. Some emboli resist lysis and may organize and persist. Occasionally, chronic residual obstruction leads to pulmonary hypertension (chronic thromboembolic pulmonary hypertension) that may develop over years and result in chronic right heart failure. When large emboli occlude major arteries, or when many small emboli occlude > 50% of the distal arterial system, right ventricular pressure increases, causing acute right ventricular failure, failure with shock (massive PE), or sudden death in severe cases. Risk factors for death include age > 70 yr, cancer, and COPD.
Pulmonary infarction occurs in < 10% of patients diagnosed with PE. This low rate has been attributed to the dual blood supply to the lung (ie, bronchial and pulmonary).
PE affects an estimated 117 people per 100,000 person years, resulting in about 350,000 cases yearly, and causes up to 85,000 deaths/yr. PE affects mainly adults.
Symptoms are nonspecific and include dyspnea, chest pain, cough, and, in severe cases, syncope or cardiorespiratory arrest. Signs are also nonspecific and may include tachypnea, tachycardia, hypotension, and a loud pulmonic component of the 2nd heart sound. Diagnosis is based on a CT angiogram, ventilation/perfusion scan, or a pulmonary arteriogram. Treatment is with anticoagulants and, sometimes, clot dissolution with thrombolytics or surgical removal.
Experiment # 4
To examine a slide showing Myocardial infarction
Here the infarct shows areas typical coagulative necrosis that typifies anoxic injury. The cells eventually lose their nuclei, lyse and are removed by scavenger cells such as monocytes. All this happened due to an ischemic event in the coronary arteries.
THEORY:
. Myocardial infarction A heart attack or acute myocardial infarction (MI) occurs when one of the arteries that supplies the heart muscle becomes blocked. Blockage may be caused by spasm of the artery or by atherosclerosis with acute clot formation. The blockage results in damaged tissue and a permanent loss of contraction of this portion of the heart muscle.
"Myocardial infarction (MI) is the irreversible necrosis of heart muscle secondary to prolonged ischemia. This usually results from an imbalance of oxygen supply and demand."
Before 6 to 12 hours: No visible lesion is seen. By 18 to 24 hours: Infarct area becomes pale to cyanotic & swollen. In the first week: The infarct area becomes progressively more sharply defined, yellow and softened. By the 7 to 10 days, circumference of the infarct area becomes hyperemic, and progressively expands. By the 6 weeks, fibrous scar is well established.
Electron microscopy shows reversible changes (swelling of mitochondria & endoplasmic reticulum and relaxation of myofibrils). Histochemically, there is loss of oxidative enzyme & fall of glycogen. In 12 to 72 hours , there is infiltration of neutrophils with progressive coagulative necrosis of myocytes. Dead myocytes become hypereosinophilic with loss of nuclei.